Understanding the invisible, systemic clinical presentations of severe developmental childhood neglect to shift therapeutic approaches from symptom-fixing to relationally-driven somatosensory co-regulation.
Q: What is the hidden clinical impact of childhood neglect on adult therapy clients?
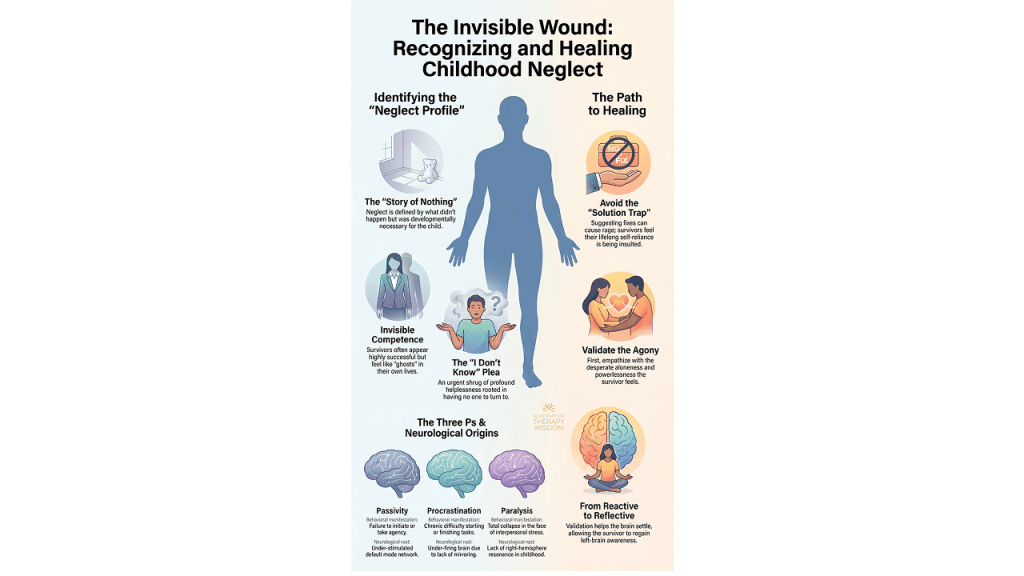
A: Childhood neglect shapes the nervous system through absence rather than overt harm, leaving adult survivors with invisible competence. Clients appear highly successful externally while struggling with profound internal emptiness, chronic paralysis, and severe relational disconnection rooted in early unmet attachment needs.

neglect, invisible competence, and nervous system adaptations.
The Story of Nothing: Recognizing the Void in Trauma Therapy
In our community of therapists, we readily recognize the flashing red flags of overt childhood abuse. We know how to map the jagged edges of intrusive trauma. Yet, some of our deepest clinical puzzles stem from a much quieter source. One of the most challenging forms of trauma to recognize is the trauma of what never happened.
Unlike abuse, childhood neglect is defined by absence rather than presence. It is a chronic lack of attunement, protection, emotional responsiveness, and co-regulation during critical developmental windows. Because there is no obvious catastrophic event to name, survivors arrive on our couches struggling to validate their own suffering. They feel broken without a reason.
When we look through a trauma-informed lens, we recognize that this structural void deeply disrupts the natural growth of neural pathways. The brain requires interactive reflection to build robust systems for self-regulation, emotional awareness, and relational safety. When the mirror is entirely blank, the developing nervous system is forced to adapt in isolation.
Invisible Competence and the Illusion of Self-Sufficiency
Many neglect survivors arrive in our offices looking exceptionally well-adjusted. They are our high-functioning executives, our hyper-independent organizers, and our deeply reliable caretakers. This presentation reflects a brilliant survival strategy known as invisible competence.

These clients have learned early on that relying on an adult leads to terrifying disappointment or dangerous vulnerability. Hyper-independence becomes their armor. They look entirely successful on the outside while carrying a crushing weight of isolation internally. As clinicians, we must look past the outer polish to touch the profound emptiness underneath.
Understanding Nervous System Adaptations in Neglect Survivors
When unmet attachment needs persist throughout early life, the physiology changes to preserve energy. What looks like procrastination, passivity, or chronic uncertainty in our adult sessions is rarely a lack of motivation. It is not clinical resistance.
These behaviors often reflect deeply ingrained neurobiological immobilization strategies. When a child cries out for comfort and encounters a wall of silence, the sympathetic nervous system’s fight-or-flight energy eventually collapses. The body drops into a dorsal vagal freeze state to protect itself from the agony of unrequited reaching.
In adulthood, when these individuals face overwhelming tasks or relational vulnerability, their physiology defaults to this ancient defense. Paralysis is not a behavioral choice; it is a somatic shield. To learn more about how somatic states dictate clinical presentation, explore our guide on somatic therapy to deepen your embodied tracking skills.
Shifting from Structural Symptom-Fixing to Relational Attunement
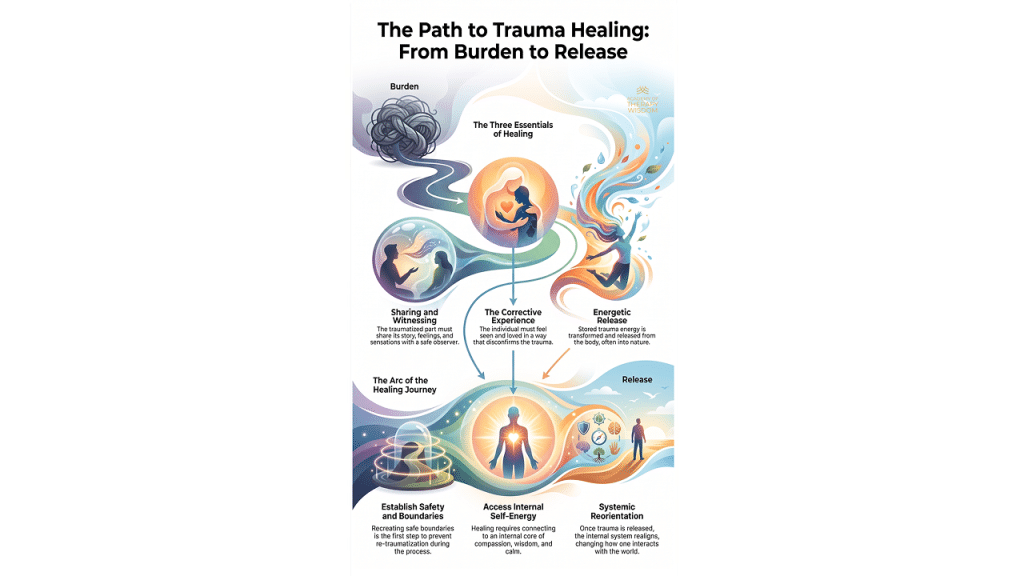
Healing the profound wounds of developmental neglect requires an intentional shift in our clinical orientation. We cannot simply offer cognitive tools or try to fix the client’s behavioral adaptations. The remedy must directly address the original injury: the absence of a resonant other.
Our primary clinical tool is our own presence. Through consistent, explicit validation and somatic resonance, we offer the nervous system a chance to experience what was missing. We provide a safe container for co-regulation, allowing the client to safely step out of chronic survival states.

This deliberate relational pacing helps move clients toward greater somatic reflection, internal integration, and authentic self-awareness. We are not teaching coping skills; we are cultivating the relational soil that allows new neural pathways to emerge. Over time, the client learns that it is safe to thaw, safe to reach out, and safe to exist without the armor of hyper-independence.
Intersecting Modalities: Tracking the Wounds of Absence
When working with deep attachment gaps, integrating multiple trauma-informed frameworks can radically enhance our efficacy. For instance, when a client presents with a severe history of early emotional deprivation, their adult personality often fragments into protective parts. One part might maintain rigid, hyper-vigilant competence while another carries the exiled, agonizing loneliness of the neglected child.
Using parts-work models can help us gently unblend these protectors without threatening the client’s internal system. Furthermore, understanding the precise physiology of safety and danger allows us to track these shifts in real-time during sessions. When we witness a client drop into a sudden flat affect or experience a loss of voice during an emotional moment, we are seeing the echo of early neglect playing out in the room.
Our job is to name these moments with exquisite gentleness, validating the body’s ancient wisdom while softly inviting a new experience of shared connection. This synthesis of parts work and nervous system tracking offers a compassionate map for navigating the complex terrain of developmental trauma. According to clinical data published by organizations like the American Psychological Association, integrated trauma treatments that address both somatic processing and relational safety yield the most sustainable recovery outcomes for complex trauma survivors.
Frequently Asked Questions
- How do I help a client see their childhood neglect if they insist their upbringing was completely normal? Clients often normalize neglect because it is the only reality they have ever known. We can gently explore their histories by focusing on the absence of emotional experiences rather than looking for overt harm. Shifting the focus to their current patterns of hyper-independence or deep internal isolation can help reveal how these ancient adaptations relate directly to early unmet attachment needs.
- What role does complex post-traumatic stress disorder play in adult survivors of chronic neglect? Chronic emotional deprivation during critical developmental windows frequently results in the development of c-ptsd, which manifests as severe emotional dysregulation, chronic toxic shame, and persistent relational difficulties. Because the trauma is relational, the recovery process must also be relational, utilizing the therapeutic alliance as a safe workshop for rewriting these old, deeply painful scripts.
- How do we differentiate between clinical depression and a trauma-informed freeze state rooted in neglect? While the outward symptoms look similar, a trauma-informed freeze state is a protective physiological defense mechanism resulting from early relational failure. By evaluating the client’s internal states through a somatic lens, we can see that their passivity is often a survival strategy designed to protect a highly sensitive system from further relational rejection.

JOIN a FREE WEBINAR TRAINING with Ruth Cohn
“Nothing Happened to Me”: Uncovering the Developmental Trauma of Neglect
In this free webinar you’ll learn:
“Nothing” Matters: Notice subtle neglect signs to avoid missing them.
Attachment is Key: Secure attachment shapes development; its lack shows in therapy.
Neglect Profile: Spot neglect via Three Ps, body language, and verbal cues.
Avoid Invalidating: Don’t dismiss helplessness or indecision to prevent distress.
Validate Experiences: Acknowledge feelings of being alone and unsupported.
Neglect-Informed Therapy: Adapt methods to address neglect, boosting effectiveness.