This post aims to provide psychotherapists with a clear framework for differentiating between neurodivergent sensory needs and trauma-driven dysregulation, offering somatic strategies for clinical application.
Q: How can therapists distinguish between neurodivergent traits and trauma responses?
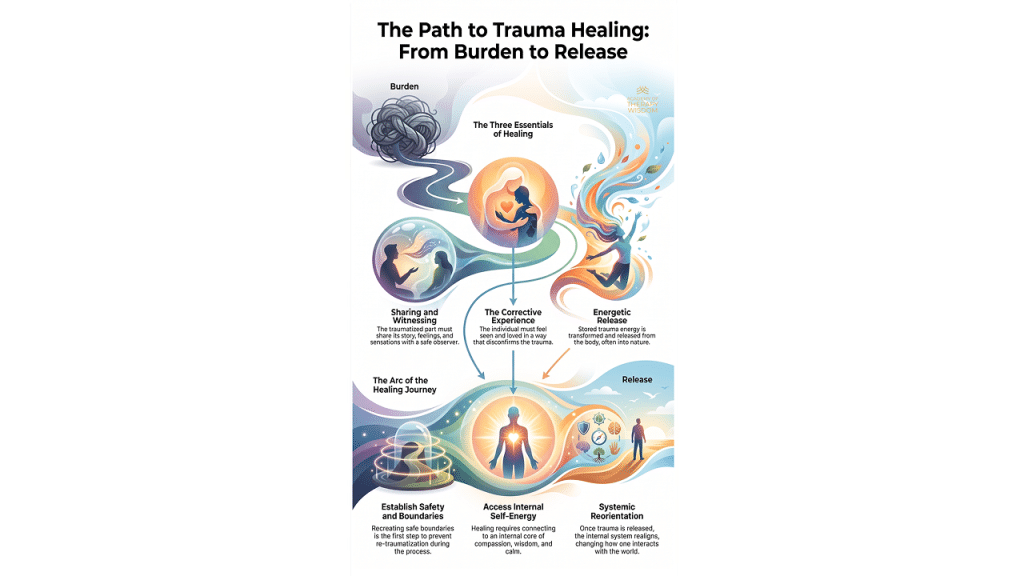
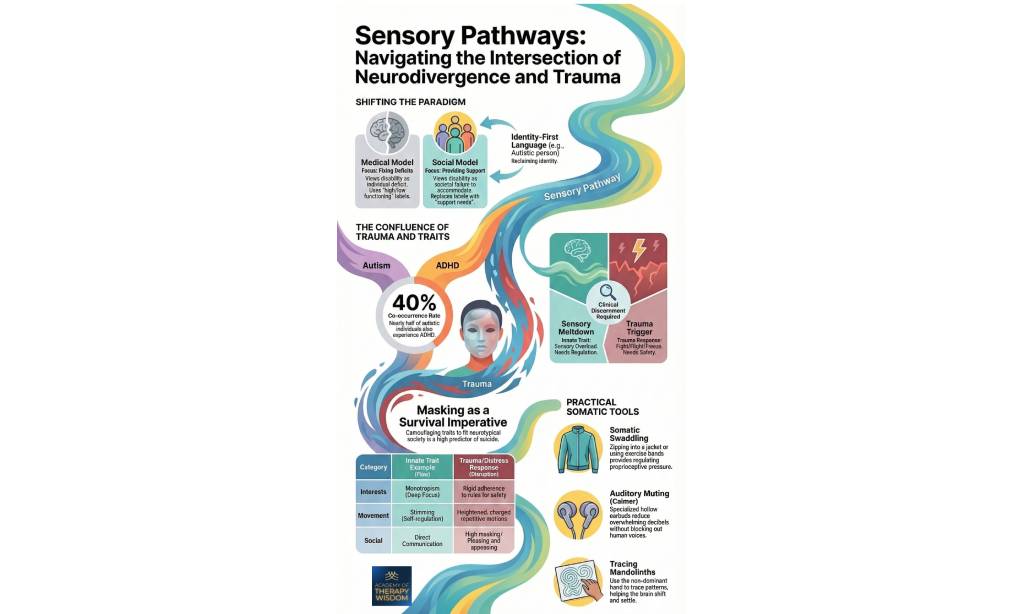
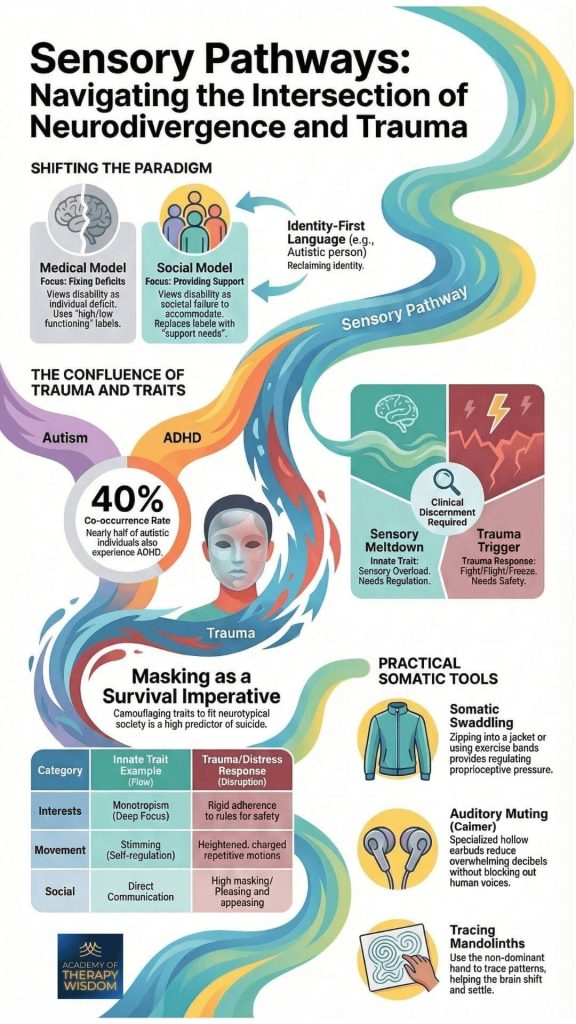
A: Clinical discernment requires shifting from “fixing deficits” to a social model of support. By identifying whether a behavior is an innate trait (like stimming for self-regulation) or a survival response (like masking for safety), clinicians can provide targeted somatic tools that honor the client’s natural sensory profile.
Shifting the Paradigm: From Deficits to Support
As therapists, we often find ourselves at a crossroads when working with neurodivergent clients who have also experienced significant relational or systemic trauma. For a long time, the medical model (focusing on fixing deficits) dominated our field. It viewed neurodivergence through a lens of individual pathology, using labels like “high” or “low” functioning that reduced a client`s agency.
What we hear from practitioners in our counseling trainings is a deep desire to move toward a social model that focuses on providing support. This shift replaces the focus on “fixing” with a focus on “accommodating.” Instead of functioning labels, we talk about support needs.
This isn’t just a change in vocabulary, it is a fundamental change in how we hold the therapeutic space. When we use identity-first language, the preference is being called an “Autistic person” rather than a “person with autism”, we are supporting a client’s right to reclaim their identity.
As Linda Thai shares in her training on nervous system regulation, the goal is not to force a client into a neurotypical standard of “calm.” Instead, we look at what the nervous system is communicating at that moment. Is the client experiencing a sensory meltdown (an innate trait resulting from sensory overload) or a trauma trigger (a survival response rooted in fight, flight, or freeze)?
The Confluence of Trauma and Traits
One of the most complex aspects of this work is the high co-occurrence rate between different neurodivergent profiles. Statistics suggest that nearly half of autistic individuals also experience ADHD, a 40% co-occurrence rate that creates a unique internal sensory landscape. According to the CDC, the prevalence of these overlapping identities means our clinical discernment must be sharper than ever.
In our partnership with experts, we’ve observed that many neurodivergent individuals navigate chronic layers of trauma simply by existing in a world not built for them. This leads to masking, a seemingly automatic act of camouflaging traits to fit into neurotypical society. Masking is not just a social habit, it is often a survival imperative. Tragically, high levels of masking are a high predictor of suicide among neurodivergent populations. When a client “pleases and appeases” in session, they may not be “doing well,” they might be stuck in a trauma-based fawning response.
To support these clients, we must understand the difference between an innate trait and a disruption. For example, stimming (self-regulatory repetitive motions) is often an innate movement that helps a client reach a state of flow. Conversely, a trauma response might manifest as heightened, charged, repetitive motions that feel frantic or out of control. One leads to regulation, the other signals a move toward the edge of the window of tolerance, that precious zone where we can process emotions effectively without feeling overwhelmed.
Practical Somatic Tools for the Therapy Room
When we look at the intersection of neurodivergence and complex PTSD, “talk therapy” often isn’t enough. We need bottom-up strategies that speak directly to the body. What we see working in the field are tools that provide a sense of self-movement and body position feedback. We call this immediate proprioceptive.
Somatic Swaddling
Zipping into a heavy jacket or using exercise bands can provide regulating pressure. This isn’t about “hiding,” it’s about providing the brain with the boundaries it needs to feel where the body begins and ends.
Auditory Muting
Using specialized hollow earbuds can reduce overwhelming decibels without blocking out human voices. This allows a client to stay engaged in the “social engagement system” while dampening the “noise” that might otherwise lead to a meltdown.
Tracing Mandolinths
Using the non-dominant hand to trace patterns helps the brain shift and settle. This simple movement can assist in moving away from a rigid, trauma-based focus (monotropism) and back into a state of present-moment awareness.
Moving Toward Liberatory Practice
Ultimately, our work is to help clients build safety without suppressing their natural needs. This involves a deep commitment to cultural humility regarding how we view “normal” behavior. It calls us to engage in a lifelong process of self-reflection and critique.
If we only see a “disordered” social style when a client uses direct communication, we miss the opportunity to celebrate their innate honesty. If we see “rigidity” where there is actually a need for safety through rules, we risk re-traumatizing the client. By integrating somatic intelligence into our practice, we can support the client’s autonomy and help them move from survival into a state of authentic self-expression.
Frequently Asked Questions
What is the difference between a sensory meltdown and a trauma trigger?
A sensory meltdown is typically an innate trait response to sensory overload, requiring immediate regulation and environment changes. A trauma trigger is a response to a perceived threat, activating a fight-flight-freeze survival state, requiring a focus on safety and grounding.
Why is identity-first language important in neurodiversity-affirming therapy?
Using identity-first language supports a client’s reclamation of their identity and moves away from the medical model of pathology. It aligns with the social model of support, emphasizing that neurodivergence is an inherent part of the person’s self-energy rather than a deficit to be cured.
How does masking impact the mental health of neurodivergent clients?
Masking, or camouflaging neurodivergent traits, is often a survival imperative in neurotypical environments but comes at a high psychological cost. Long-term masking is a significant predictor of burnout, exhaustion, and even suicide, often complicating the treatment of attachment disorder or chronic trauma. Treatment encourages what is called earned secure attachment, which lowers the occurrence of masking.
What are proprioceptive tools in somatic therapy?
Proprioceptive tools, like somatic swaddling or weighted blankets, provide the nervous system with deep pressure input that helps define body boundaries. These tools are effective for clients experiencing dissociation or sensory dysregulation, as they help the brain “locate” the body in space and time.
What you´ll learn:
- Vestibular Engagement for Emotional Regulation
- Using the Eyes to Hack the Stress Response System
- Subtle Sounds to Release the Peri-Trauma Response
- Effective Self-Holding and Self-Swaddling Techniques
- How and When to Apply Bilateral Stimulation
- Integration and Completing the Stress Response Cycle