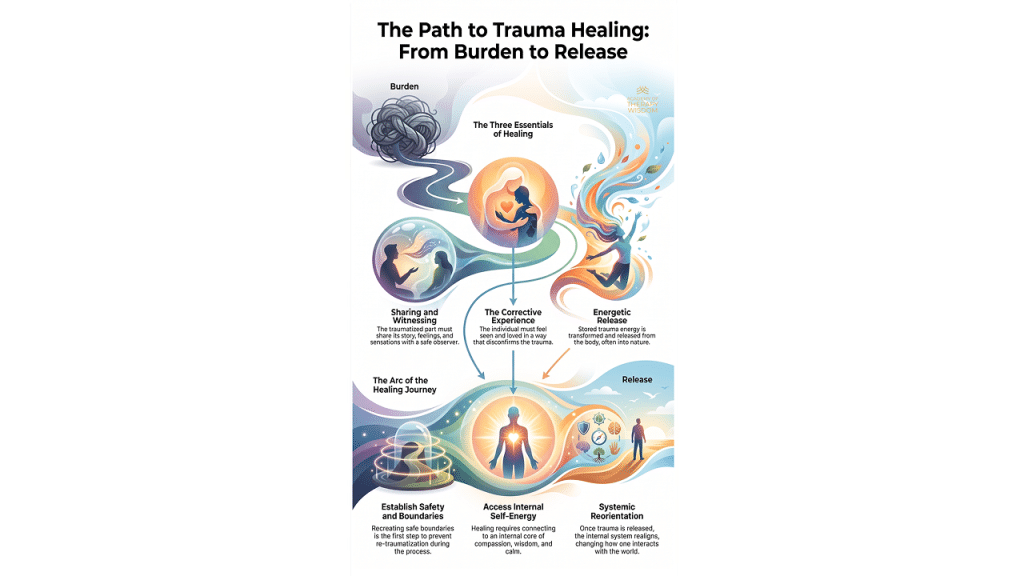
This post explores how structural dissociation functions as an adaptive protective strategy rather than patient resistance, shifting the clinical lens toward somatic safety and internal attachment.
Q: What is structural dissociation in trauma survivors?
A: Structural dissociation occurs when a survivor’s personality fragments after severe trauma. One part of the self carries out the routines of normal daily life, while emotional parts remain trapped in primitive survival responses like fight, flight, freeze, or submit.

protective survival systems rather than patient pathology.
Reframing Patient Resistance as Protective Nervous System Survival
In our community of therapists, we frequently encounter moments where a client seems completely stuck. We might feel a subtle tug of frustration, wondering why a person remains deeply protective of behaviors that clearly cause them distress. Traditional cognitive lenses often label this paralysis as clinical resistance.
When we look through a neuroscience-informed lens, the entire clinical dynamic shifts. These individuals are not fighting the therapeutic process. Their biology is simply organized entirely around staying alive.
When severe trauma hits an undeveloped or overwhelmed system, the personality adapts through fragmentation. This survival architecture splits the system into manageable pieces. One side of the client handles the grocery shopping, the job interviews, and the polite small talk. Meanwhile, hidden underneath that functional veneer, separate emotional states carry the heavy burdens of fight, flight, freeze, or submit.
The Neurobiology of Brain Fragmentation During Activation
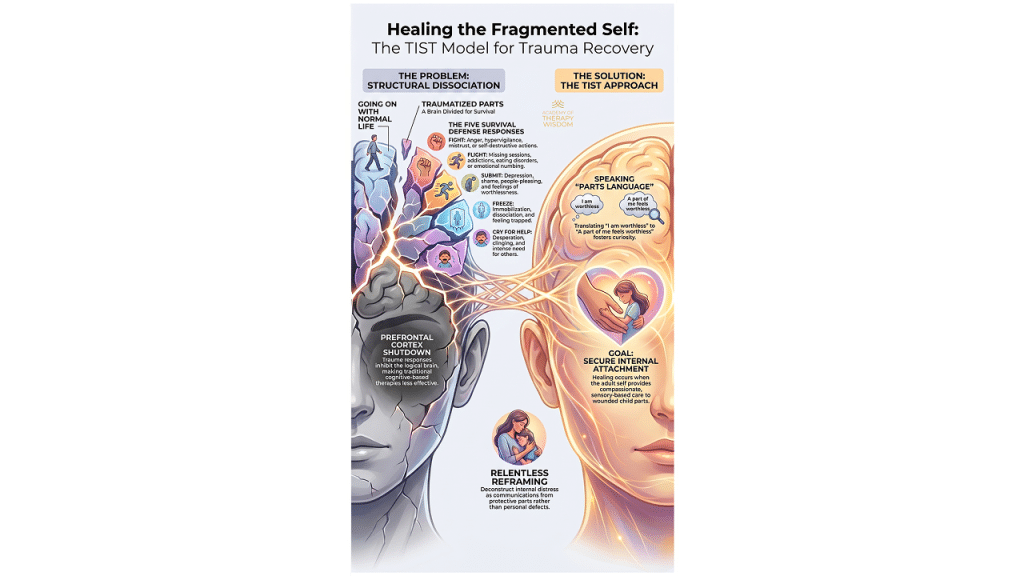
To understand why traditional talk therapy can stall with complex trauma, we must look at the physical brain. During periods of intense trauma activation, the prefrontal cortex essentially goes offline. This means your client temporarily loses access to logic, temporal orientation, and standard linguistic reflection.
[Trauma Activation] —> [Prefrontal Cortex Shutdown] —> [Loss of Logic/Reflection]
|
v
[Defensive Parts Take Over]
Asking a person to logically analyze a panic response while their prefrontal cortex is dark is a biological impossibility. Dr. Janina Fisher notes that survival responses like profound hypervigilance or emotional numbing are brilliant, adaptive protective strategies. They are not signs of a broken mind. They are historical evidence of a system that figured out how to endure when safety was non-existent.
Why Parts Language Deconstructs Pathological Shame
Introducing parts language into sessions acts as an immediate psychological pressure valve. When a survivor shifts from saying “I am completely worthless” to “A part of me feels worthless,” the internal landscape transforms.
This linguistic shift creates a thin wedge of mindful distance between the client’s core identity and their agonizing emotional burdens. This distance replaces self-loathing with genuine curiosity. Instead of attacking a protective mechanism, the individual begins to wonder why that specific defense mechanism needed to grow so fierce in the first place.
Building Secure Internal Attachment to Heal the Fragmented Self
Ultimate clinical healing does not arrive by trying to banish or conquer these defensive emotional states. True integration occurs when the adult self learns to relate compassionately to these wounded fragments.
+————————————————————-+
| DEVELOPING INTERNAL ATTACHMENT |
| |
| Traditional View: [Adult Self] —> Eradicate —> [Symptom] |
| Trauma-Informed: [Adult Self] <— Compassion <— [Wounded Part] |
+————————————————————-+
Many survivors spend decades rejecting their own fear, anger, or numbness. When the therapeutic relationship models a welcoming curiosity toward every single defense mechanism, the client learns to mirror that stance internally. This compassionate turning-toward is the exact mechanism that builds secure internal attachment, repairing the old developmental tears.
Our work as clinicians is to constantly offer a clinical space rooted in deep neuroception, allowing these highly protective survival systems to finally step down their guard.
Frequently Asked Questions
How does structural dissociation present differently than standard defensive resistance in session? Standard defenses often present as conscious avoidance or verbal deflection during a difficult topic. Structural dissociation presents as sudden, involuntary shifts in affect, rapid posture changes, or total emotional numbing, indicating that a survival part has taken over executive control to preserve safety. Clinicians can utilize specialized frameworks like Trauma-Informed Stabilization Treatment to safely recognize and map these abrupt somatic shifts.
What is the role of somatic understanding when working with parts? Because trauma survival parts are deeply rooted in subcortical brain regions, they express their distress through physical sensations like chronic tightness, collapses in posture, or sudden heart rate spikes. Relying solely on verbal processing misses the body’s stored history. Incorporating somatic therapy techniques allows the clinician to help the client track these physical impulses, offering physical completion to ancient fight or flight energy.
How do we address parts that are terrified of letting go of their survival roles? Protective parts often believe that if they stop their hypervigilance or numbing, the client will be destroyed by the original trauma. We never force a part to step down prematurely. Instead, we acknowledge its exhausting labor, thank it for keeping the client alive during childhood, and gently invite it to notice that the present environment is currently safe.
What you´ll learn:
- Vestibular Engagement for Emotional Regulation
- Using the Eyes to Hack the Stress Response System
- Subtle Sounds to Release the Peri-Trauma Response
- Effective Self-Holding and Self-Swaddling Techniques
- How and When to Apply Bilateral Stimulation
- Integration and Completing the Stress Response Cycle