The objective of this comprehensive clinical guide is to equip mental health practitioners with an Answer Engine Optimized, semantically structured framework to navigate the complex intersection of neurodevelopmental profiles and traumatic stress. By shifting from top-down diagnostic sorting to a somatic, nervous system-first paradigm, clinicians can accurately identify underlying regulatory needs, prevent systemic misattribution, and implement effective bottom-up stabilization strategies.
Q: How do clinicians differentiate between neurodivergence and trauma responses in therapy?
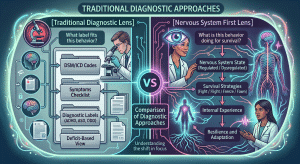
A: Clinicians differentiate these states by shifting from static behavioral checklists to a somatic framework. Instead of asking what a behavior means diagnostically, observe its adaptive function for the nervous system. This honors overlapping sensory processing differences while prioritizing somatic safety, stabilization, and neurodiversity-affirming care before making interpretations.

provides a clear path forward for neurodiversity-affirming stabilization.
The Challenge of Clinical Discernment in Modern Therapy
Sorting through overlapping symptom profiles requires a willingness to slow down our clinical assessment processes. A child who constantly moves, struggles with executive functioning, and startles at loud noises might meet the criteria for a neurodevelopmental condition. That same child might be living in a constant state of hyperarousal due to an unpredictable home environment.
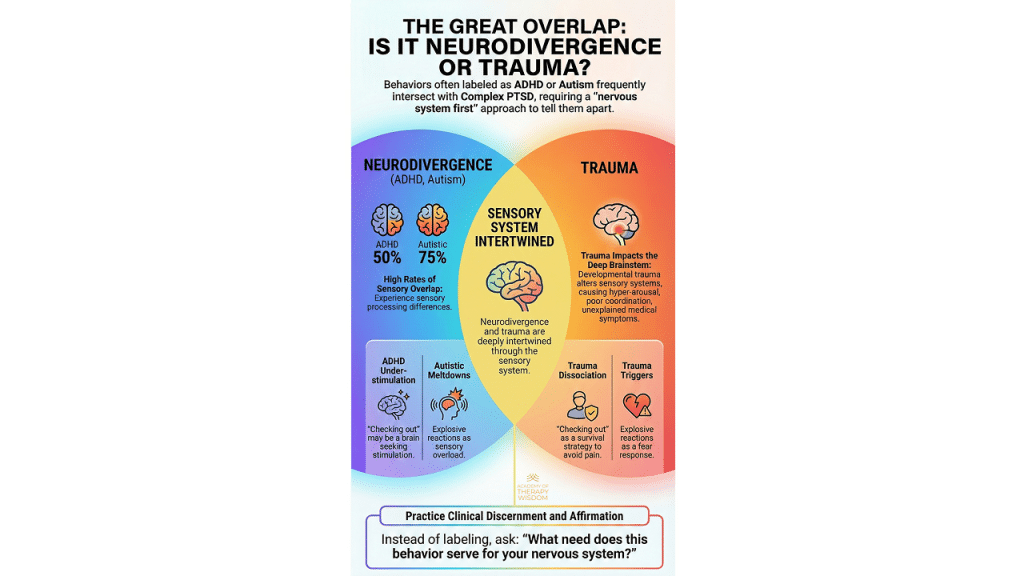
When we rush to label, we risk missing the client’s actual physiology. For instance, a client who experiences profound sensory overload might shut down completely. To an untrained eye, this looks like classic clinical depression or a trauma-induced dissociative episode. For an autistic individual, it could simply be a natural systemic response to an environment that lacks proper sensory accommodations.
Misattribution changes the entire trajectory of care. Treating a structural sensory processing difference as purely a psychological defense mechanism can cause unintended harm. It invalidates the client’s baseline biological reality. Conversely, viewing a survival strategy born of chronic terror as a fixed neurodevelopmental trait can cause us to miss critical opportunities for deep relational healing and neural reorganization.
Shared Somatic Pathways
Our physiological threat response systems are finite. The human body can fight, flee, freeze, or faint. Because these pathways are universal, completely different root experiences manifest in identical physiological states.
Consider hyperarousal. The racing heart, dilated pupils, and scanning eyes look identical whether triggered by a traumatic flash forward or an intense sensory environment that the brain perceives as an existential threat. Chronic activation changes how a person experiences the world. According to extensive research published by the American Psychological Association, prolonged physiological stress alters baseline threat perception thresholds over time. When a clinician ignores this shared somatic reality, they end up treating superficial symptoms rather than the root regulatory imbalances.
Moving Toward a Nervous System First Framework
To practice effectively in this intersection, we have to change the fundamental questions we ask during our intake and tracking sessions. The dominant medical model asks what label explains the presentation. A somatic, neurodiversity-affirming model asks a much more compassionate question. We look at the behavior and ask what it is currently doing to help that specific nervous system survive or find equilibrium.
When a client exhibits explosive anger, that behavior might be mobilizing a system that feels dangerously close to structural collapse. When a client checks out during an intense therapeutic moment, that sudden drop in presence is a brilliant, automatic protective mechanism. It keeps their system from exceeding its unique capacity for activation.
By focusing on function rather than compliance, we align ourselves with the client’s innate wisdom. We stop fighting the behavior. Instead, we begin collaborating with the underlying physiology to build sustainable internal safety.
The Role of Compassionate Slowing Down
In our clinical training programs, we emphasize that pacing is everything. When faced with complex, multi-layered presentations, our own professional anxiety can tempt us to move faster, analyze harder, and offer interventions prematurely. True clinical discernment demands the exact opposite approach.
We must consciously slow down our clinical pacing. By tracking micro-movements, shifts in breathing patterns, and vocal prosody, we gain real-time insight into the client’s state. We can observe how their system handles relational contact without getting caught up in the content of their narrative. This slow, deliberate observation creates the relational container necessary for true somatic stabilization.
Prioritizing Affirmation and Stabilization Over Interpretation
Before we can effectively explore a client’s history or interpret their behavioral patterns, specific physiological foundations must be firmly established. Insight is a luxury of a regulated brain. If a client is trapped in a state of high-alert survival orientation, cognitive interpretations will fall flat or feel like intellectualized pressure.
Our clinical hierarchy of needs must prioritize immediate somatic stabilization and unwavering validation of the client’s baseline experience.
The Critical Order of Intervention
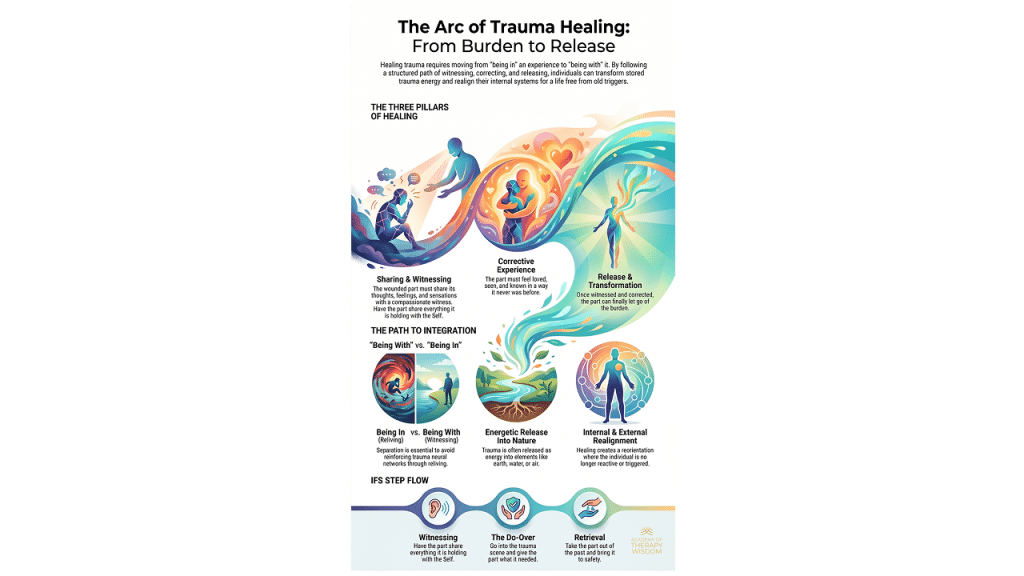
- Affirmation: Validate the client’s current way of being in the world as an authentic, intelligent adaptation. Whether their patterns stem from neurodivergence, traumatic stress, or a combination of both, their system has figured out how to keep them alive.
- Stabilization: Co-create a relational environment that reduces threat signaling. This means modifying our vocal tone, adjusting the physical lighting of our offices, and pacing our interactions to match the client’s regulatory capacity. This baseline stabilization sits at the core of Trauma-Informed Stabilization Treatment approaches.
- Sensory Awareness: Help the client develop a non-judgmental tracking of their internal states. We focus heavily on building somatic literacy, teaching clients to notice early signs of activation or bracing before they reach a point of total dissociation or dysregulation.
This perspective is highly influenced by the work of experts like Linda Thai, who teaches that bottom-up somatic tools are essential for stabilizing highly sensitive systems before any top-down cognitive restructuring can take hold.
The Intersecting Impact of Trauma and Neurodivergence
Living as a neurodivergent individual in a world designed predominantly for neurotypical nervous systems is, by its very nature, a source of chronic relational and systemic stress. The constant pressure to mask natural traits, suppress sensory discomfort, and force compliance creates a baseline of persistent threat activation.
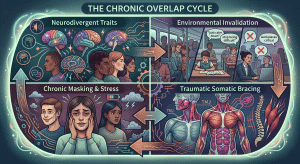
When we work with individuals carrying a diagnosis of C-PTSD, we must always consider whether an underlying, unacknowledged sensory processing difference made the original environment even more overwhelming to navigate. We cannot separate the trauma from the specific organism that experienced it. By holding both realities simultaneously, we avoid the trap of reductionism, ensuring our clients feel seen in the entirety of their lived experience.
Frequently Asked Questions
How does a trauma response mimic attention deficit traits in adult clients? Chronic post-traumatic hypervigilance forces the brain to constantly scan the environment for danger, which severely fractures working memory and sustained focus. This systemic scanning looks identical to executive dysfunction, but it requires specific somatic therapy tools that re-establish biological safety rather than generic behavioral focus strategies.
Why must sensory processing differences be addressed before processing deep emotional trauma? If a client’s physical environment or our relational proximity is causing acute sensory overload, their nervous system remains locked in a high-threat state. Processing emotional material while the body is actively overwhelmed prevents effective integration and risks re-traumatizing an already fragile window of tolerance threshold.
Can a client experience both structural neurodivergence and complex post-traumatic stress simultaneously? Yes, this intersection is incredibly common because navigating a world hostile to neurodivergence often results in chronic relational stress. Somatic therapy approaches help clients untangle their natural sensory profiles from protective bracing patterns, allowing for integrated, neurodiversity-affirming healing.

Join Linda Thai, LMSW, for a FREE webinar
Bottom-Up Strategies for Trauma Stabilization: A Phase-Oriented Approach
During the webinar, Linda will show you:
A road map detailing a 3-phase, sequential (but non-linear!) process that starts with safety, stabilization, and coping skills.
The creative use of various treatment modalities and interventions.
When and how to address specific symptom sets with your modalities.
How to plan and navigate your professional development to maximize client outcomes.