Understanding the Trauma Continuum: A Resilience-Informed Perspective
Q: What is a resilience-informed approach to trauma?
A: A resilience-informed approach defines trauma as an internal nervous system response that overwhelms a person’s coping capacity. It prioritizes the presence of wellbeing and relational connection over the mere absence of symptoms, helping clinicians pace interventions based on the client’s current regulatory needs.

Redefining Trauma and Resilience in Clinical Practice
In our community of therapists, we often find that the traditional medical model focuses heavily on the “absence of disease.” However, when we partner with experts like Arielle Schwartz, we see a vital shift toward viewing health as the “presence of wellbeing.” This fundamental change transforms how we sit with the humans in front of us in the therapy room.
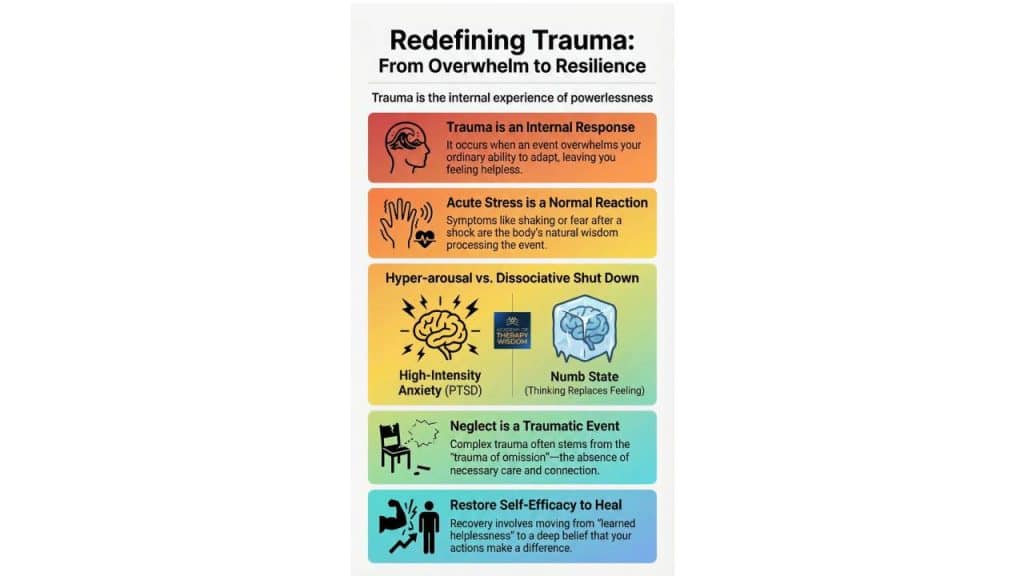
When we talk about trauma as “overwhelm,” we are describing a moment where ordinary human adaptations are pushed past their limits. This can leave a client feeling fundamentally powerless. What we hear from practitioners in our training is that the most profound way to alleviate this stress is through the relational resource—simply feeling “not alone” in the suffering. By focusing on what we call self-efficacy, we move away from a deficit-based model and toward one of empowerment.
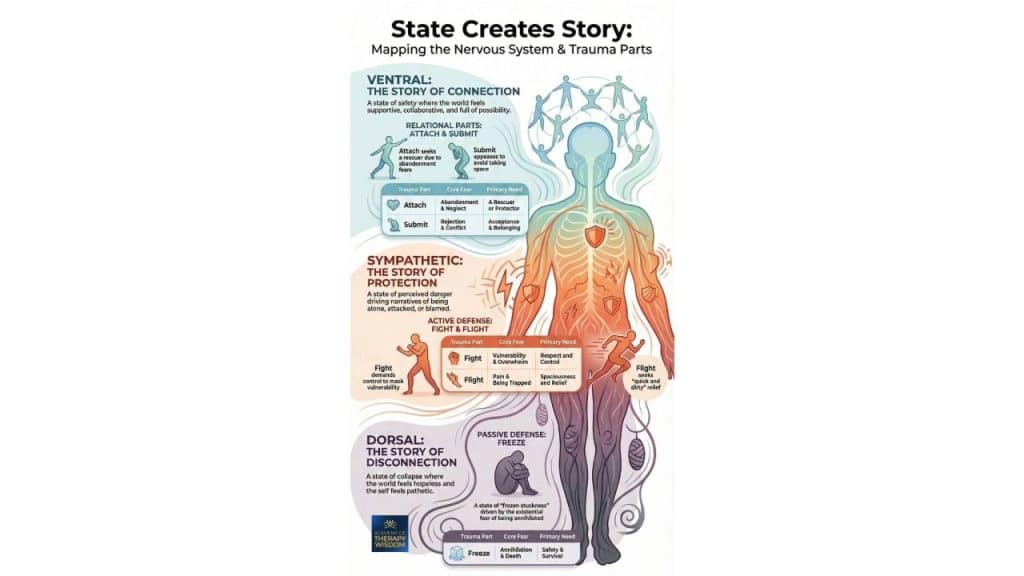
The Tiers of Traumatic Stress: A Nervous System Map
Tracking the timeline and the biological “flavor” of a client’s distress is vital for effective treatment. As shown in the infographic, we generally categorize these into distinct tiers based on intensity and duration.
Acute Stress and Healthy Processing
Initial symptoms following a shock are often a normal, expected biological response. In our community, we advocate for clinicians to de-pathologize these early reactions. Within the first month, the nervous system is often still trying to process the event through its natural regulatory cycles.
Hyperarousal vs. Dissociative Shut Down
If symptoms persist, we begin to track two primary survival states:
- Hyperarousal: This state is dominated by high emotional tension, panic, and fight-or-flight activation. The brain’s alarm center—the amygdala—is often driving the system here.
- Dissociative Shut Down: Conversely, this state involves numbness or a “shut down” of feelings. The prefrontal cortex may become overactive in an attempt to intellectually defend against overwhelming emotions.
The Trauma of Omission: Recognizing Neglect
We must not overlook the reality that neglect—the trauma of what didn’t happen—can shape complex trauma in profound ways. This trauma of omission often leads to deep difficulties with affect regulation and interpersonal connection.
Clinical Application: Pacing and Self-Efficacy
What we hear from practitioners is that the key to avoiding therapist burnout is pacing. We must ask: where is the client’s current capacity for neuroception—the nervous system’s subconscious detection of safety?
As Arielle Schwartz shares in her training, our own therapeutic-presence is one of the most powerful tools for co-regulation. If we can stay grounded, we help the client stay within their window-of-tolerance, which is the zone where emotions can be processed without the system shutting down.
Research holds up what we see in our offices every day. For example, a significant study featured in The Lancet Psychiatry emphasizes that the strength of the therapeutic alliance is a core predictor of success in trauma-focused work. It is not just about the technique; it is the safety of the connection that allows for neuroplasticity to take hold. When we prioritize this bond, we create a container where healing becomes a shared, lived experience.
Frequently Asked Questions
How can I help a client understand the difference between hyperarousal and shut down? Begin by helping them track the “speed” of their internal experience. Hyperarousal feels like a racing heart or high-speed thoughts, while shut down feels like being “stuck” or heavy. Using a somatic-therapy lens, you can help them name these states as biological protection rather than personal failure.
Why is relational connection considered a resource in trauma therapy? Trauma often happens in isolation. Feeling “not alone” acts as a biological counter-signal to the brain’s alarm system. Restoring this connection is a core part of healing attachment-disorder and building the safety necessary for deeper trauma processing.
What is the role of self-efficacy in resilience-informed care? Self-efficacy is the felt sense that one’s actions can create change. Trauma frequently involves a loss of this sense. Part of the healing arc is moving from learned helplessness toward active participation in one’s own regulation and life choices.
What you´ll learn:
- Vestibular Engagement for Emotional Regulation
- Using the Eyes to Hack the Stress Response System
- Subtle Sounds to Release the Peri-Trauma Response
- Effective Self-Holding and Self-Swaddling Techniques
- How and When to Apply Bilateral Stimulation
- Integration and Completing the Stress Response Cycle