Exploring the neurobiological failure of narrative encoding and the rise of somatic storage in trauma survivors.
Q: Why is trauma often remembered as sensations rather than a clear story?
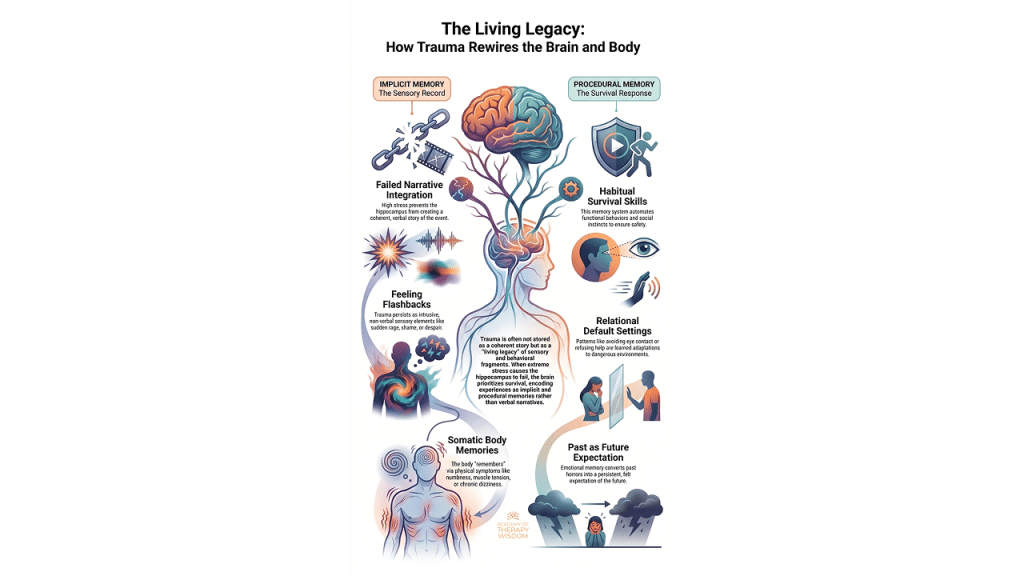
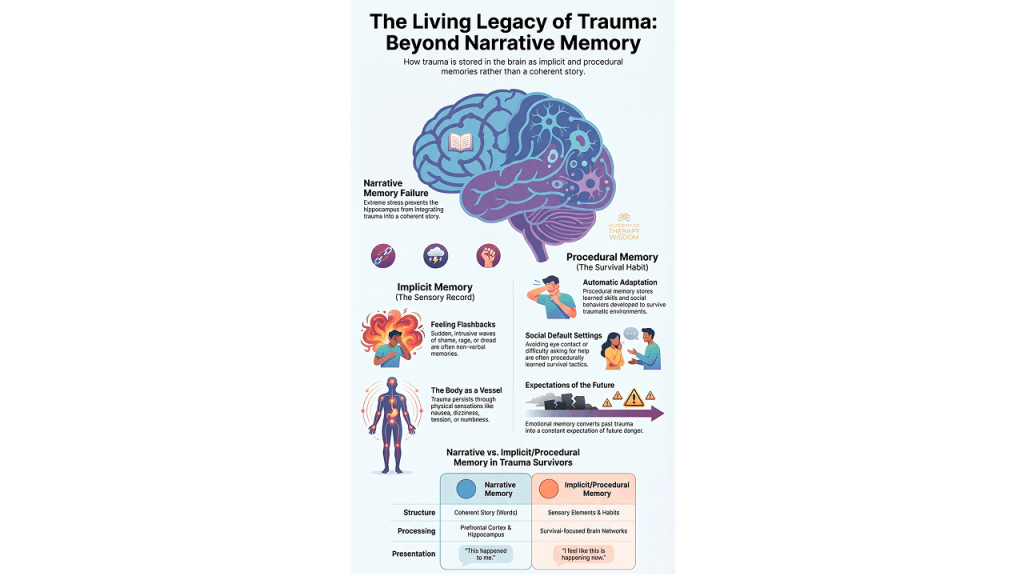
A: During high stress, the hippocampus struggles to organize events into a narrative. The brain prioritizes protection, shifting storage to implicit and procedural systems. This leaves the survivor with sensory fragments, emotional waves, and survival habits instead of a coherent verbal memory.

encoded as a sensory and physical record rather than a narrative.
Beyond the Narrative: The Silent Language of Survival
In our community of therapists, we frequently encounter clients who feel like they are failing at therapy because they cannot tell us exactly what happened. They come to us with gaps in their history. They bring us feelings they cannot name. We know that trauma does not always sit in the brain as a clear story with a beginning, middle, and end.
The neurobiology of this is fascinating and quite forgiving when we explain it to our clients. When things get overwhelming, the hippocampus basically hits a wall. This part of our brain usually acts like a librarian, filing away our life events with a date and time stamp. But during a crisis, the librarian leaves the room. The brain shifts focus entirely to the amygdala and survival systems. It chooses protection over storytelling every single time.
The Sensory Record of Implicit Memory
Because the narrative filing system fails, the memory has to go somewhere else. It lands in our implicit memory system. This is what many of us call the sensory record. It doesn’t have words. It doesn’t have a timeline. Instead, it surfaces as “feeling flashbacks.”
A client might be sitting in their kitchen and suddenly feel a wave of sheer dread or a hot spike of shame. They look around and see no reason for it. This is the body remembering. These are non-verbal emotional records that were never fully integrated into the life story. As clinicians, we have to help clients understand that these sensations are actually memories. They are just speaking a language that doesn’t involve the prefrontal cortex. Working with somatic therapy allows us to listen to this language without needing the client to “explain” it.
Survival Habits and Procedural Memory
The body also learns how to stay safe through procedural memory. Think of this as the “survival habit” system. The brain encodes behaviors that once worked to keep the person alive or safe. This might look like avoiding eye contact, keeping the shoulders tight, or an inability to ask for help.
These adaptations are often the very things that bring people into our offices. They find these patterns are now interfering with their current relationships. It is helpful to remind them that these aren’t personality flaws. They are automatic adaptations stored in the nervous system. When we look through the lens of polyvagal theory, we see that the body is just following a safety manual it wrote years ago. We cannot simply talk someone out of a procedural memory. We have to work with the body to update the manual.
Working with Fragmented Parts of the Self
When trauma is stored this way, the person often feels fragmented. They have “parts” of themselves that feel and act differently than their conscious, adult self. Dr. Janina Fisher has taught us so much about how to work with these fragmented parts of trauma survivors. These fragments are often holding the weight of those unintegrated sensory memories.
If we stay purely at the cognitive level, we miss the heart of the pain. The dissociation that many survivors experience is a direct result of these memory systems being disconnected. Our goal is to move beyond the “why” and start looking at the “how” of their experience. By focusing on the neurobiology of how the body holds these records, we can help our clients find a sense of safety that doesn’t depend on having all the answers to their past. This is the path toward genuine neuroplasticity and lasting change.
Frequently Asked Questions
Why does my client feel shame about not remembering their trauma? Clients often believe that a lack of narrative memory means they are making it up or being “difficult.” In reality, hippocampal impairment during trauma is a common biological response to extreme stress. You can find more details on this in our C-PTSD overview.
How do you treat memories that have no words? Treating non-verbal memories requires somatic and experiential interventions. Instead of asking what happened, we focus on the neuroception of the client—how their body is sensing danger in the present moment. This helps regulate the system so integration can eventually occur.
Can procedural survival habits actually be changed? Yes, though it takes more than cognitive insight. Because these habits are stored in the procedural memory system, we use body-based practices to create new experiences of safety. This helps move the client into a state of self-energy where they can choose new responses.
What you´ll learn:
- Vestibular Engagement for Emotional Regulation
- Using the Eyes to Hack the Stress Response System
- Subtle Sounds to Release the Peri-Trauma Response
- Effective Self-Holding and Self-Swaddling Techniques
- How and When to Apply Bilateral Stimulation
- Integration and Completing the Stress Response Cycle