This post aims to educate mental health practitioners on the nuanced differences between acute stress, PTSD, and C-PTSD while advocating for a resilience-informed, relational approach to trauma recovery.
Q: What is a resilience-informed approach to trauma?
A: A resilience-informed approach defines trauma as an internal nervous system response that overwhelms coping capacity. It prioritizes the presence of wellbeing, relational connection, and self-efficacy (the belief in one’s ability to succeed) over a simple absence of symptoms, helping clinicians pace interventions based on the client’s regulatory needs.
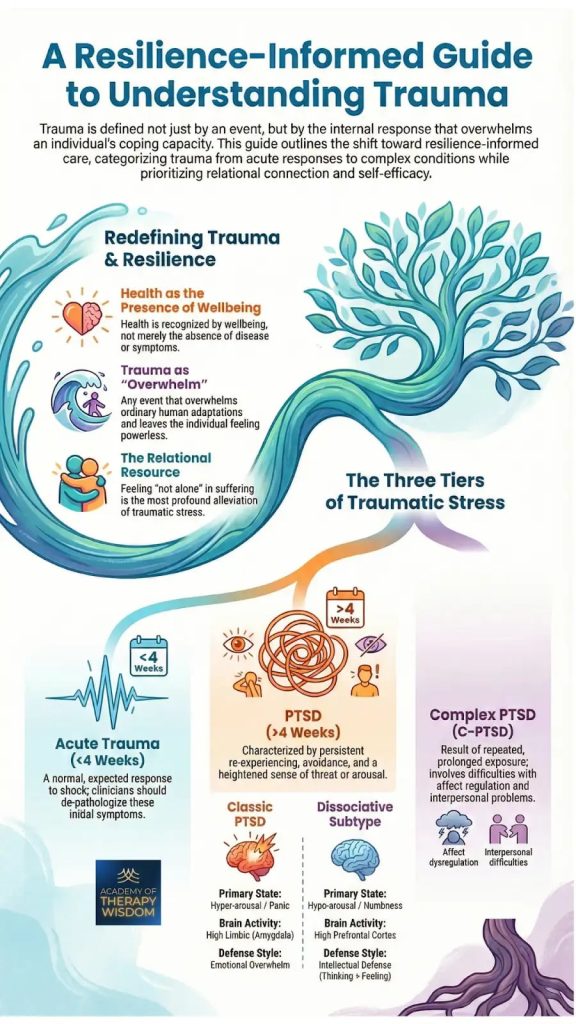
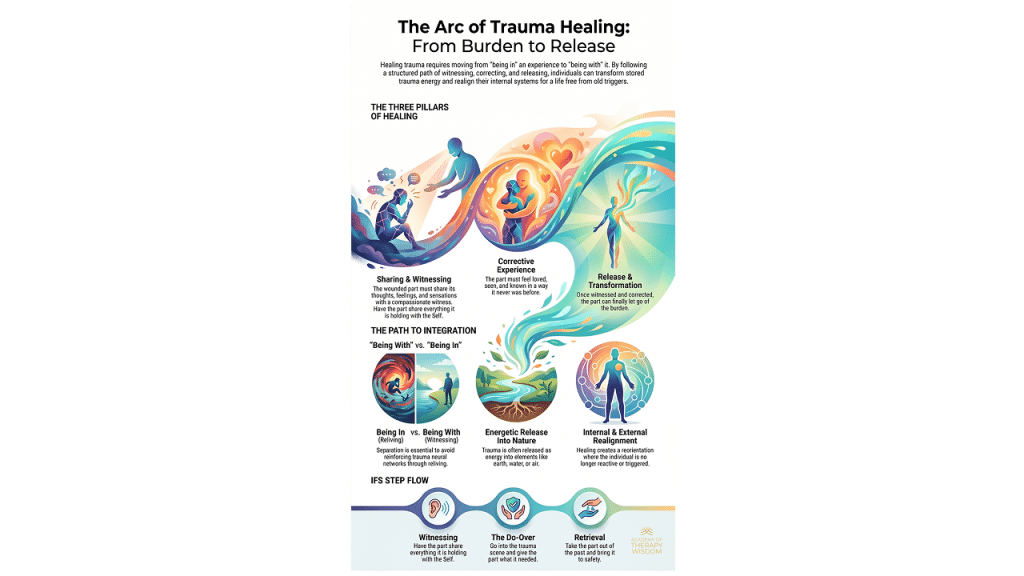
Redefining Trauma and Resilience in Clinical Practice
In our community of therapists, we often find that the traditional medical model focuses heavily on the “absence of disease.” However, as we partner with experts like Arielle Schwartz, we see a vital shift toward viewing health as the “presence of wellbeing.” This essentially changes how we sit with the humans in front of us in the therapy room.When we talk about trauma as “overwhelm,” we are describing a moment where ordinary human adaptations are pushed past their limits. This can leave a person feeling powerless. What we hear from practitioners in our training is that the most profound way to alleviate this stress is through the relational resource, -simply feeling “not alone” in the suffering. By focusing on what we call self-efficacy, we move away from a deficit-based model and toward one of empowerment.
The Three Tiers of Traumatic Stress: A Nervous System Map
Understanding the timeline and the biological “flavor” of a client’s distress is vital for effective treatment. We generally categorize these into three distinct tiers:
Acute Trauma (Under 4 Weeks Since the Event)
When a shock occurs, the initial symptoms are often a normal, expected biological response. In our community, we advocate for clinicians to de-pathologize these early reactions. Within this first month, the nervous system is often still trying to process the event.
PTSD (Over 4 Weeks After the Event)
If symptoms like persistent re-experiencing, avoidance, and a heightened sense of threat last longer than a month, we begin to suspect and assess for Post-Traumatic Stress Disorder.
What is particularly interesting for clinicians is the distinction between two primary states:
- Classic PTSD: This is dominated by hyper-arousal (a state of high emotional and physical tension) and panic. The brain activity is centered in the “high limbic” system, specifically the amygdala, the brain’s alarm center.
- Dissociative Subtype: Here, the primary state is hypo-arousal (a state of very low energy) or numbness. The brain shows higher activity in the prefrontal cortex as it attempts an “intellectual defense” to shut down overwhelming feelings.
Complex PTSD (C-PTSD)
When trauma is not a single event but the result of repeated, prolonged exposure, we see complex-ptsd. This involves deep difficulties with affect regulation (the ability to manage emotional states) and significant interpersonal problems. This is where the layers of attachment and systemic issues often intersect, requiring a slow, steady approach to rebuilding the “relational resource.”
Clinical Application: Pacing and Regulation
What we hear from practitioners is that the key to avoiding the emotional residue of exposure to others’ trauma, what we commonly refer to as vicarious-trauma, and client retraumatization is pacing. We must ask: where is the client’s current capacity for neuroception (the nervous system’s sub-conscious detection of safety or danger)?
As Dr. Arielle Schwartz shares in her training on therapist burnout, our own therapeutic-presence is one of the most powerful, if not THE most powerful, tools for co-regulation. If we can stay grounded, we help the client stay within their window-of-tolerance, that the zone where emotions can be processed without the system shutting down or exploding.
Research holds up what we see in our offices every day. For example, a significant study featured in The Lancet Psychiatry (a leading clinical journal) emphasizes that the strength of the therapeutic alliance—the collaborative bond between you and your client—is a core predictor of success in trauma-focused work. It isn’t just about the “technique,” but the safety of the connection that allows for neuroplasticity (the brain’s ability to reorganize itself by forming new neural connections) to take hold. When we prioritize this bond, we create a container where healing becomes a shared, lived experience rather than a clinical goal.
Frequently Asked Questions
What is the difference between hyper-arousal and hypo-arousal in trauma?
Hyper-arousal is a “fight or flight” state characterized by panic and high limbic activity, while hypo-arousal is a “freeze or faint” state involving numbness and dissociation. Understanding which state a client is in helps a therapist choose the right tools for somatic-therapy to bring the nervous system back to balance.
Why is relational connection considered a “resource” in trauma therapy?
Trauma often happens in isolation or through the betrayal of a relationship. Feeling “not alone” acts as a biological counter-signal to the brain’s alarm system. Restoring this connection is a core part of healing attachment-disorder and building the safety necessary for deeper trauma processing.
How does a resilience-informed lens differ from a traditional diagnosis?
A traditional diagnosis focuses on symptoms and “what is wrong,” whereas a resilience-informed lens looks at what the nervous system is trying to protect. It prioritizes somatic-intelligence (the wisdom of the body’s sensations) and seeks to restore the client’s self-efficacy rather than just suppressing their symptoms.
What you´ll learn:
- Vestibular Engagement for Emotional Regulation
- Using the Eyes to Hack the Stress Response System
- Subtle Sounds to Release the Peri-Trauma Response
- Effective Self-Holding and Self-Swaddling Techniques
- How and When to Apply Bilateral Stimulation
- Integration and Completing the Stress Response Cycle